
Potassium & The Heart: Hypo/Hyperkalemia
Introduction
Electrolytes - at their simplest explanation - are nutrients, vitamins, and minerals responsible for assisting in the structure of our body and the regulation of metabolic body processes. They can be either derived from our diet, produced naturally within the body, or a combination of both. They are essential for the maintenance of life and health - and as such, it is critical for EMS providers to understand the pathophysiology behind them when handling patient cases. Electrolytes are especially important for the conduction of the heart. One of the major life threats that prehospital providers may treat is hyperkalemia and potassium imbalances.
Potassium (K)
Potassium is one of the most well-covered electrolytes in the national Paramedic curriculum. Potassium is found in a variety of foods, including bananas, fruits, and beans. Potassium serves as a cation, meaning positively charged ion, to provide muscle contractions and nervous conduction. Paramedics are routinely called to address potassium issues in the context of dialysis patients. Normal potassium lab values are between 3.0mmol/L and 5.0mmol/L.
Hypokalemia is defined as lab potassium levels below 3.0mmol/L, with severe hypokalemia being diagnosed at levels below 2.5mmol/L (Castro and Sharma, 2022). Hypokalemia is seen less often in patients, but still can constitute a clinical emergency. Major causes for hypokalemia include severe dehydration, excessive exercise without electrolyte supplementation, and poor diet habits. Some medications, especially psychiatric medications, can put patients at risk for hypokalemia development (Castro and Sharma, 2022). Hypokalemia can also be seen with ESRD patients post-dialysis, as the process of dialyzing can deplete potassium levels temporarily. Patients in a state of acute alkalosis may also develop hypokalemia as a compensatory mechanism as potassium shifts to intracellular areas (Sur and Mohiuddin, 2021).
Patients experiencing severe hypokalemia may present with muscular weakness with dominant symptoms in large leg muscles, respiratory depression, lethargy, and bradycardia. Long term hypokalemic patients are also at increased risk for rhabdomyolysis and renal failure conditions, further complicating the dialysis patient population.
EKG changes of hypokalemia include bradycardia, QT interval prolongation, and the development of a prominent “U” wave in place of normal T waves. Patients experiencing hypokalemia have decreased cardiac automaticity, and are thus at risk of developing escape and ventricular rhythms as a result.

Image sourced from American Journal of Medicine. Prominent U waves can be seen developing in V2 and V3 on this 12Lead EKG.
Patients that are suspected for hypokalemia will need close cardiac monitoring and continuous reassessment. Patients may also require education regarding frequent follow-up with their primary care providers following new medications, maintaining an adequate diet tailored to their health challenges and medication prescriptions, and understanding their increased risk in the event of a fall. Prehospital providers can jumpstart patient care by obtaining a comprehensive history including medications, diet, and recent life events, obtaining vascular access and blood sampling, continuously monitoring and handing off 12Lead EKG findings, and completing a full, thorough physical assessment. Patients with hypokalemia secondary to dehydration may also require intravenous fluid administration. Decisions to treat possible dehydration should be made in conjunction with physical skin turgor findings and history information.
Potassium replacement therapies are best done in the hospital during in-patient stays. Oral routes are often opted for over intravenous replacement because of the risks involved with a rapid rise of potassium levels (Castro and Sharma, 2022).
Hyperkalemia is a more common prehospital emergency. Hyperkalemia is diagnosed at potassium levels above 5.5mmol/L, with the severity of symptoms increasing with serum potassium levels. Severe hyperkalemia levels constitutes a clinical emergency and can sometimes be treated prehospitally depending on jurisdictional protocols. Patients with renal failure or dialysis treatments and rhabdomyolysis make up some of the most common patient populations that hyperkalemia occurs in prehospitally.
Like all muscles in the body, the heart works off the sodium-potassium ion pump. This is a metabolic process that continually maintains a resting negative state inside of muscle cells, with contractions occurring because of a sudden influx of (positive) sodium ions. This depolarizes the muscle cell and causes contraction occur. Following a contraction, the muscle cells return to a polarized, negative internal resting state. With hyperkalemia, the
Hyperkalemia symptoms include lethargy, muscular weakness, respiratory depression, and bradycardia. In many ways, the symptoms of extreme hyperkalemia mimics the symptoms of extreme hypokalemia. Understanding disease pathologies and conducting a good assessment will help providers choose between the two in the field. Hyperkalemia is commonly seen in patients that have missed dialysis for an extended period of time. Patients who have missed dialysis and become emergent are usually lethargic, weak, and clearly sick when assessed.
If left untreated and at extreme levels, hyperkalemia can lead to the development of dangerous cardiac arrhythmias. As hyperkalemia progresses, a gradual lengthening of the QRS complex can be observed. This can begin in the precordial V leads, but can show up anywhere on a 12Lead. As it progresses, hyperkalemia will progress into a ventricular rhythm and become progressively more chaotic. Ventricular fibrillation is the end rhythm of most patients, compromising perfusion and leading to cardiac arrest.
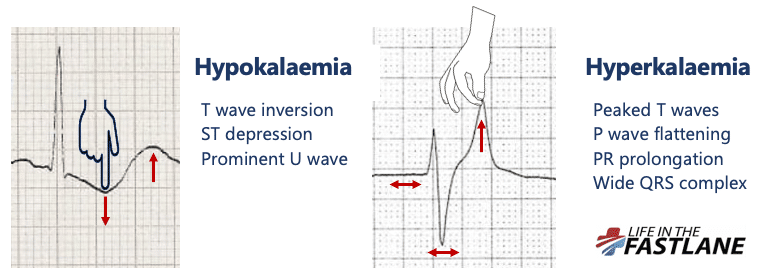
Image sourced from Life in the Fast Lane (Butner and Burns). The image right shows the progression of peaking T waves seen in hyperkalemia.
Field treatment of hyperkalemia focuses on early recognition, continual cardiac monitoring, and obtaining a comprehensive history of the patient. Some jurisdictional protocols allow for the administration of calcium chloride, usually in 0.5 to 1 gram doses, for hyperkalemia control. Calcium works by stabilizing the myocardium and reversing the erratic depolarizations that hyperkalemia can cause (Lederer, 2022). Some protocols also allow for sodium bicarbonate administration for control of acidosis in hyperkalemic patients. Other treatments commonly provided for longer term treatment of hyperkalemia include Albuterol, insulin, Kayexalate, and dialysis. All treatments primarily focus on shifting potassium within the body to reduce overall blood serum levels and combat acidosis.
Works Cited
Buttner, R., & Burns, E. (2021, June 2). Hypokalaemia. Life in the Fast Lane . Retrieved February 4, 2022, from https://litfl.com/hypokalaemia-ecg-library
Castro, D., & Sharma, S. (2021, July 20). Hypokalemia. StatPearls [Internet]. Retrieved February 4, 2022, from https://www.ncbi.nlm.nih.gov/books/NBK482465
Eleanor Lederer, M. D. (2021, December 14). Hyperkalemia. Practice Essentials, Background, Pathophysiology. Retrieved February 2, 2022, from https://emedicine.medscape.com/article/240903-overview>
Sur, M., & Mohiuddin, S. (n.d.). Potassium. National Center for Biotechnology Information. Retrieved January 29, 2022, from https://pubmed.ncbi.nlm.nih.gov/30969613/>